Breast Cancer Diagnosis in 36 Hours or Less?
How PINC AI Applied Sciences, GE and St. Luke’s University Health Network Came Together to Adapt a One-Stop Breast Clinic Model for the United States
In the U.S., it takes an average of 28 days between the time a woman has an abnormal screening mammogram and receives a biopsy; 31.6 days for the first surgeon visit; and 52.6 days for breast surgery, with far higher delays for women of color. This, in turn, leads to significant anxiety and stress for women and their families, and may even affect prognosis. But how do we reduce this gap between screening mammograms and pathology?
GE Healthcare, in partnership with Gustave Roussy Cancer Center in Villejuif, France, thought they had the answer. GE had been working with the Breast Cancer Department at Gustave Roussy in Paris, where Dr. Suzette Delaloge invented the concept of rapid diagnosis in the One-Stop Clinic. The One-Stop Breast Clinic (OSBC) model was designed to provide patients with a coordinated journey in one location from the initial appointment through diagnosis and treatment plan, with one team, in one day.
The French model used fine needle aspiration (FNA), colocation of services and equipment to expedite diagnostic screening to pathology and results. They worked to internationalize the One-Stop Clinic, and in 2017, opened an OSBC in Medellin, Colombia, and now have four additional clinics in Bogota, Barranquilla, Bucaramanga and Cali.
In 2018, GE approached Premier’s PINC AI Applied Sciences team asking the question, “How could we partner to build an OSBC in the U.S.?” There were a few hurdles to overcome; for starters, FNA is not an accepted practice in the U.S. National Comprehensive Cancer Network (NCCN) guidelines, meaning the team couldn’t adopt the full French model. They would have to adapt and redesign the model to fit the U.S.
Instead of “No,” PINC AI Applied Sciences Said, “How?”
It would have been easy to say “no” when the team realized that the model wouldn’t fit NCCN guidelines, but they didn’t. The PINC AI Applied Sciences (PAS) team conducted a rapid evidence review, which included a comprehensive evaluation of expedited diagnoses for patients with breast cancer in the U.S.
Utilizing PINC AI Healthcare Data (PHD), they were able to verify that women can wait as long as 21 days to receive a diagnosis from a diagnostic mammography. This is 21 days in addition to the time the woman waited prior to scheduling, completing a mammography screening, scheduling and completing a diagnostic mammography, and finally waiting for results. The evidence was sobering. With early detection still one of the most important processes that can impact short- and long-term outcomes, closing the gap between screening and pathology was obvious.
Identifying a Partner
PAS identified a potential pilot hospital, St. Luke’s University Heath Network (SLUHN), because they had better-than-average results and reduced wait times. They quickly met with GE to examine the French model and how it could translate into a U.S. model. The SLUHN team was represented by Dr. Joseph Russo and Michele Brands from the SLUHN Regional Breast Center. Both Dr. Russo and Michele recognized right away that a U.S. model would require an entire reconfiguration of imaging operations. From scheduling to diagnosis and everything in between, there was room to improve the process.
After the collaborative meeting, GE partnered with PAS to engage SLUHN in a pilot project. Recognizing that the reality of a same-day diagnosis without FNA would be nearly impossible, the team set out to produce an OSBC model that used core needle biopsy and could result in a 36-hour or less diagnostic screen-to-diagnosis process.
Adapting the Model
PAS was uniquely positioned to verify the delay in breast cancer diagnosis using robust data to show the lag exists, and to confirm U.S. literature. PAS recognized the work in France was nothing short of amazing, but U.S. guidelines inhibited a model replication. The team took the opportunity to work with GE, an industry partner, and SLUHN, a Premier member, to define how to move forward and create clinical change.
PAS and SLUHN worked to understand the reasons for a delay in turnaround time (TAT) and response rates, and to find out where changes could make the most impact. During the analysis, PAS was able to confirm the literature that states breast cancer diagnosis TAT is woefully slow. The team was focused on ways to test and challenge the SLUHN team to reduce time from mammography screening to pathology and diagnosis.
“Making an improvement in clinical care requires understanding the care pathway and all operations that are needed to support it,” said Roni Christopher, Vice President of Design and Implementation for PAS. “When the processes are clearly defined, providers and care teams can operate with consistency and success. People can be reluctant to make changes or work toward improving something if the path to get there isn’t clear. This project relied on both quantitative and qualitative data to inform our approach. Our work with SLUHN and GE was about designing good processes, gathering feedback from many stakeholders, including staff and patients, and then adopting them.”
PAS worked with SLUHN to support GE to redesign practice workflow based on data and feedback from SLUHN executives, clinical leaders, administrative leaders, schedulers, care coordinators, ultrasound techs, lab services and community members.
They mapped the current process and identified opportunities for improvement. They recognized that scheduling, lab courier services and staff commitment would be key cornerstones in creating and embracing this new model of care. The SLUHN team had consistent support from their system leaders, and Michele Brands, Dr. Joseph Russo and Dr. Karl Yaeger provided the department leadership required to ensure that an effort like this would reach its goal.
The team considered everything from clinical workflows, patient engagement strategies, IT supports, job descriptions and staff skills to the placement and location of equipment, the patient’s overall experience and how to replicate changes from the main regional hub to other regional centers.
Model Implementation
Since 2008, SLUHN had been working to streamline its TAT for mammography screening to pathology. They had implemented a hub-and-spoke model that allowed for central control of policies and procedures while creating a similar experience at other regional centers. If any woman seen in its 20 screening clinics needed a second-level screening or diagnostic workup, she went to a consolidated center where clinicians, technologists and nurses worked together to offer a same-day biopsy to the highest-risk patients.
“SLUHN has always been an early adopter of innovation in technology, workflow and patient experience,” said Michele Brands, Network Director of Women’s Imaging at SLUHN. “We constantly seek ways to reduce the woman’s anxiety, and that has been our guiding light since starting this journey. We’re constantly holding ourselves to a high standard with regards to quality, patient experience and turnaround times.”
By 2019, they had slashed the time between screening and pathology from 28 days to 11 days and the time between diagnostic imaging and pathology to five days. They felt this time was still too long, especially if a woman received results before a weekend, adding additional days before a biopsy could be performed.
This led SLUHN to highly consider the OSBC model. They took on this initiative during the COVID-19 pandemic, which highlighted the importance for this type of redesign. During COVID-19, when shelter-in-place orders caused healthcare facilities to cancel all elective procedures, SLUHN operated the OSBC two days a week for women with palpable lesions who could not delay care. Once orders were lifted and patients returned to completing preventive screenings, SLUHN saw an increase in advanced cancers. This new One-Stop model provided a way to triage and move these critical patients through the system swiftly.
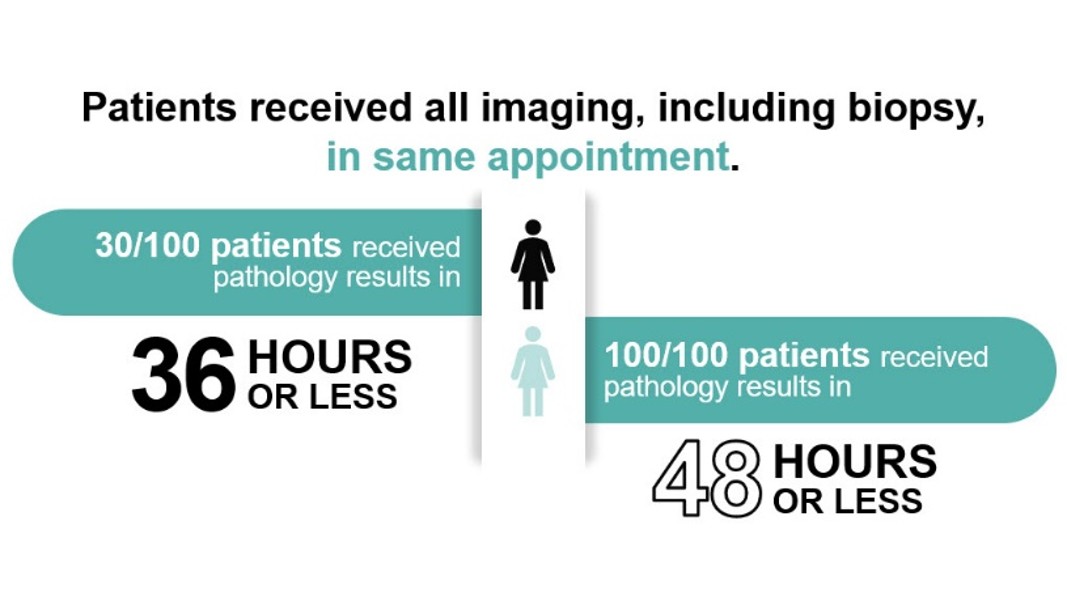
As of October 2021, the SLUHN team had seen its 100th One-Stop patient. Of those seen in this model, 30 percent of them were diagnosed within 36 hours and 100 percent within 48 hours.
Considering the Patient Experience
Patient experience was always at the center of the work. The team considered how they would message, schedule, share results and follow up with One-Stop Clinic patients. They knew they needed to engage the patients and help them become informed healthcare consumers. When patients are engaged and have more control in the process, their anxiety can be reduced. It’s not enough to tell a patient they need to do something; we have to match our instructions to a patient’s style, and better understand where they are in their decision-making process. Clinicians can be effective with small changes in their words, their follow-up and how they set expectations.
“I’ve always told the team, our silent goal is to look at every single patient as an individual, and think about their emotional state,” said Michele. “She could be a mom or a grandmother who is now leaving our facility to pick up her children. We must provide individual clinical care while also emotionally supporting each patient individually.”
PAS used the 3Is Framework, a tool developed by the PAS team that helps design rapid cycle changes to close gaps in care. The Framework helped to organize SLUHN’s approach for applying care pathways and focusing on process change that would yield improved patient outcomes. They started by helping to identify the right patient population and the people in the health system who need to understand why they should be focused on certain types of patient outreach in a timely manner. Then they helped the SLUHN team understand how to intervene during all aspects of the new care pathway. Lastly, the team adopted new strategies to interact with patients in an empathetic manner while enhancing efficiency in the process. This helped the team become purposeful about providing the right care at the right time. This leads to patients entering the system feeling like their care is prioritized.
Individualized care is at the core of oncology, but early detection and rapid diagnosis is about managing populations. It’s about proactive, preventative interventions that create an opportunity for the patient to work in partnership with their provider on a long-term plan for well-being. The U.S. model provides a comprehensive approach to breast cancer screening and diagnosis that creates a One-Stop experience for the patient’s entire care plan.
Future steps involve adding contrast-enhanced spectral mammography (CESM) to the One-Stop Clinic to help visualize dense breast tissue and help improve the time from pathology to surgery. Other health systems have expressed interest in this model, and there is opportunity to expand and adapt it to other therapeutic areas.
PAS continues to use implementation science techniques and process redesign workflows to test solutions, research and provide real-world data to help members and partners launch or advance their efforts. PAS strives to help develop, teach, test and research care delivery practices through real-world interventions and prospective research and clinical trials to help improve patient outcomes.
The team has created a suite of materials, the One-Stop Toolkit, to help others choose the One-Stop approach to care. Find out more by contacting PremierStudies@premierinc.com.
Learn more about PINC AI Applied Sciences and the power of the PINC AI Healthcare Data.





