PINC AI™ Data:
CMS Data Underestimates Hospital Labor Spending

The following article was written by Blair Childs, Senior Vice President of Public Affairs, and Aisha Pittman, MPH, Vice President, Policy, Premier Inc.
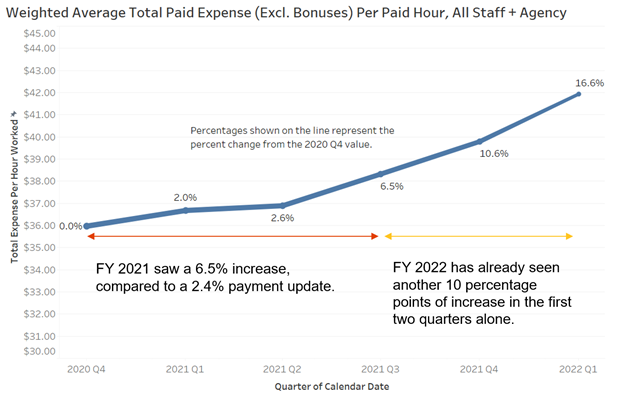
CMS updates hospital rates based on a wage inflation index that represents historical data. For FY 2021, this resulted in hospitals receiving only a 2.4 percent rate increase, compared to a 6.5 percent increase in hospital labor rates, according to PINC AI™ data. Labor costs account for 76 percent of hospital costs.
For FY 2022, CMS’s estimates of hospital spending growth using historic data represented less than half the actual growth in the prices paid by hospitals for labor, supplies and services.
The data CMS uses to account for real inflation in the cost of labor and other expenses is unlikely to reflect reality and produce an accurate payment update for the FY 2023 IPPS rule, due this spring.
Later this spring, the Centers for Medicare & Medicaid Services (CMS) is expected to release proposed rules for the Inpatient Prospective Payment System (IPPS). For the FY 2021 and FY 2022 rules, CMS applied upward payment adjustments of 2.4 and 2.7 percent, respectively.
However, a recent PINC AI™ analysis finds that CMS’s payment adjustments did not adequately address hospitals’ increased costs. According to new data, hospitals’ labor rates alone jumped 16.6 percent on a per-paid-hour basis since Q4 2020 (start of government FY 2021) and do not show signs of slowing. Labor makes up about 68 percent of the CMS market basket calculation used to adjust hospital payments. A very high payment update in FY 2023 will be needed to match the rates most acute care providers are now paying their staff.
Importantly, these costs do not appear to be exclusively COVID-19 pandemic-related or transitory. Long before the pandemic, many clinical staff were in short supply and growing closer to retirement age. According to pre-pandemic research published in 2018, healthcare was projected to be short more than 1 million nurses by 2020 as a result of nurse retirements, an aging U.S. population and a stagnant talent pipeline. Since that time, the pandemic has only exacerbated matters, with more than 500,0000 nurse retirements expected in 2022. In fact, latest research from JOLTS/BLS indicates that there are 2.7 open positions for every one position filled. As talent shortages become more severe, providers are paying more to attract and retain scarce staff, a reality that is not expected to slow down as the pandemic subsides.
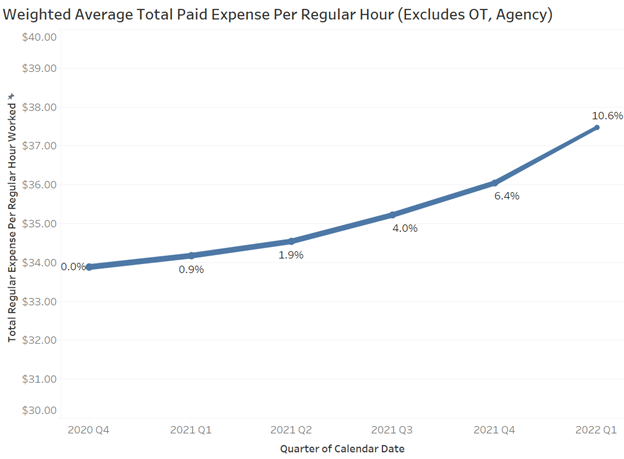
In fact, even removing use of temporary agency labor and overtime expenses that may have been more readily used to manage pandemic surge, inflation for labor expenses is still up 10.6 percent in 2022.
Moving into the third year of the pandemic, our nation’s hospital and health system workers have cared for more than 4 million COVID-19 patients. At the same time, patient acuity and length of stay have increased when compared to earlier in the pandemic. These challenges are compounded by ongoing delays in non-emergent procedures and increased costs for supplies, medicine, testing and protective equipment.
Exacerbating the problem is the fact that relief from the 2 percent sequestration cuts has also expired, replaced by 1 percent cuts from April to the end of June, followed by a full resumption of the cuts by July 1. The net effect would be to add insult to injury – holding payment to below the actual increases in costs when many acute care providers are struggling to stay afloat after years of COVID-related financial losses.
As a result, it is imperative that CMS and Congress take action to ensure hospitals are adequately compensated. CMS should account for these expenses appropriately as part of its proposed IPPS rule update, due sometime this spring. Congress should also place a moratorium on the sequester, make additional provider relief funds available and provide additional time to spend provider relief funds previously distributed.
Methodology: To determine changes in hospital labor expense rates, PINC AI™ analyzed the data within its workforce optimization solutions, one of the nation’s largest and most robust sources for geographically diverse productivity data and benchmarks – all collected and validated by health system users daily. Paid Expense (Excluding Bonus) and Paid Hours figures are provided to PINC AI™ by its client health systems. The database of more than 1,400 hospitals was filtered to include only hospitals that provided both of these figures accurately for the same quarter, resulting in a representative sample of 580 hospitals across 110 health systems. For each quarter, the sum of Paid Expense (Excluding Bonus) was divided by the sum of Paid Hours, resulting in the Weighted Average Paid Expense Per Paid Hour figure shown in the chart. The value of this figure for each quarter was compared to the value for the initial quarter (Q4 2020) to calculate a percentage increase.
Paid Expense (Excluding Bonus) includes the wages for all salaried and hourly employees, including overtime but excluding bonus and other incentive payments. Expenses paid for contracted employees are included if provided by the health system. Paid Hours includes all worked, vacation, sick and other PTO hours for which the worker was paid. These two figures, and the resulting Weighted Average Paid Expense Per Paid Hour figure, provide the most direct comparison to the Employment Cost Index (ECI) used by CMS when determining the percentage change in hospital per-unit labor costs for the annual IPPS payment update. For FY 2023 IPPS proposed rule, the ECI data will include historical data through Q4 2021 and forecasted data for Q1 2022. The final rule will use updated data that includes historical data through Q1 2022 and forecasted data for Q2 2022.
 Blair Childs
Blair Childs
Senior Vice President of Public Affairs
Blair is the primary spokesperson and communications strategist for the organization on key issues impacting healthcare costs and quality. He serves as liaison to the U.S. Congress, White House, healthcare policymakers and other major bodies involved in healthcare policy and regulation. Based in Washington, D.C., Blair leads Premier’s advocacy and thought leadership units, and is a member of Premier’s Executive Team.
 Aisha Pittman, MPH
Aisha Pittman, MPH
Vice President, Policy, Premier
Aisha leads Premier’s advocacy efforts on provider reimbursement, including quality measurement and alternative payment models.





